Pulmonary interventions

Safe localization of pulmonary nodules
We developed the Lung Marker System for use in surgical video-assisted thoracoscopic procedures (VATS). VATS procedures, smaller and non-superficial nodules are often difficult to find. The SOMATEX Lung Marker enables the safe and precise marking of such pulmonary nodules. The risk of conversion from a VATS procedure to an open thoracotomy due to inaccurate or erroneous marking is reduced.
Lung Marker System
Reduced risk of conversion in VATS procedures
The Lung Marker System is used for the preoperative marking of smaller, non-palpable intrapulmonary nodules. We have developed the localization wire specifically for use in surgical video-assisted thoracoscopic procedures (VATS) such as VATS lobectomies. Accurate localization of the nodule is a decisive factor in conducting successful VATS procedures.
- Precise localization of pulmonary nodules
- Secure and stable marking
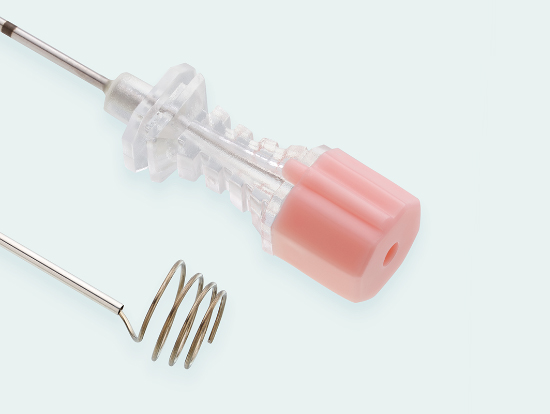
- 18 G puncture cannula with stylet
- Spiral wire for secure anchoring in tissue
- Marking with pinpoint accuracy – no unintended marking of surrounding tissue, as can be the case when using dye marking
- Lung Marker can be pulled back into the cannula and released again
Comparison of clinical results for the SOMATEX® Lung Marker System against other localization techniques (especially hook wires)
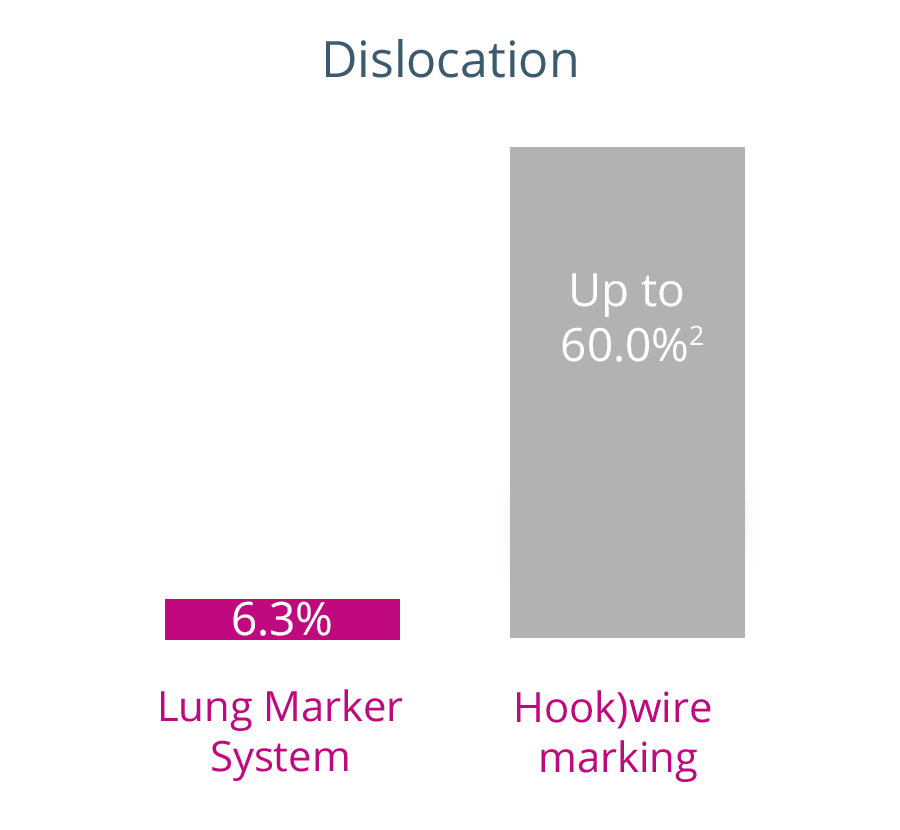
In contrast to other common lung marking techniques, the Lung Marker System has been designed for use in surgical video-assisted thoracoscopic procedures (VATS). A comparison of clinical results with the Lung Marker System against those of other localization techniques shows significantly lower complication rates .
*Source: Partik et al., Using a dedicated Lung-Marker System for localization of pulmonary nodules before thoracoscopic surgery, AJR Am J Roentgenol. 2003; 180: 805-809.
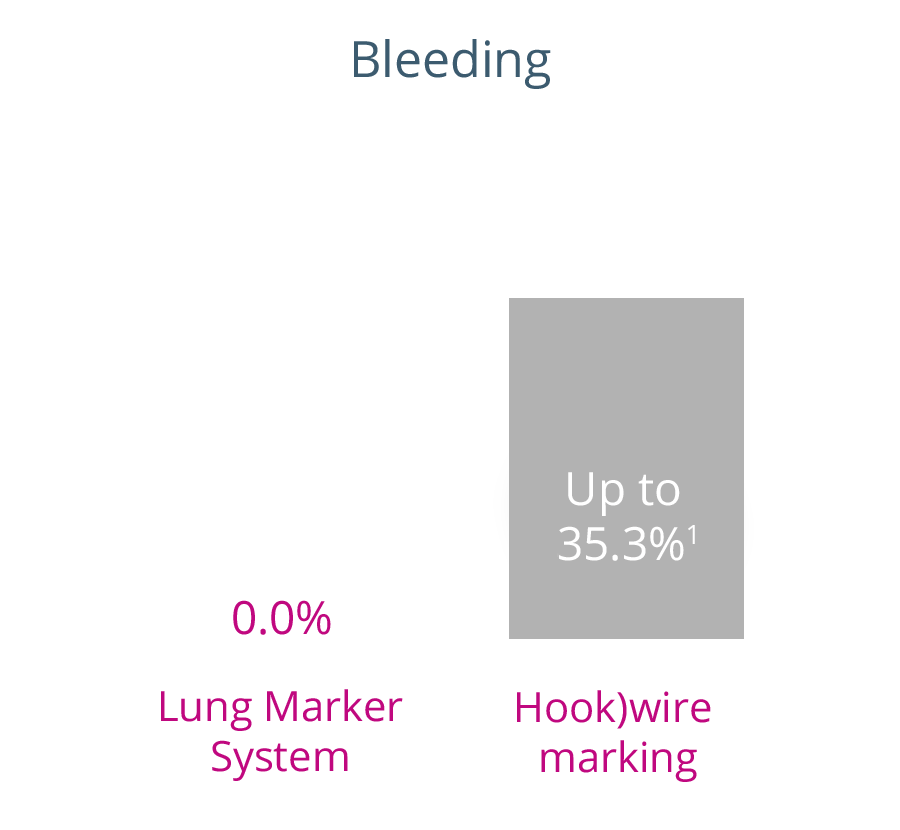
1Clinical results in the literature between 6.9% and 35.3%
2Clinical results in the literature between 6.0% and 60.0%
Lung Marker System conversion rate due to incorrect marking
n
133
224
245
Conversion rate
0.0%3
4.5%4
0.0%5
Source
3Torre et al., Chest 2004; 125: 2289-2293.
4Eichfeld et al., Ann. Thorac. Surg. 2005; 79: 313-317.
5Hänninen et al., Acta Radiol. 2004; 45: 284-288.
Dislocation rate of SOMATEX® Lung Marker System
Dislocation rate
2.3%6
3.3%7
4.0%8
6.3%9
Source
6Hirschburger et al., Thorac. Cardiov. Surg. 2008; 56: 106-109.
7Schulze et al., Fortschr Röntgenstr 2012; 184: 535-541.
8Hänninen et al., Acta Radiol. 2004; 45: 284-288.
9Partik et al., AJR Am J Roentgenol. 2003; 180: 805-809.
Localization
Precise localization of pulmonary nodules reduces the risk of conversion in VATS procedures

Stability
Secure and stable marking reduces the risk of complications
Repositioning
Lung Marker can be pulled back into the cannula and released again
Lung marker in CT

Lung marker in CT
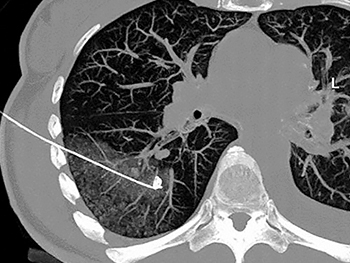
Lung marker in CT
Scientific publications
“The combination of CT-guided nodule fixation with spiral wire and the subsequent thoracoscopic resection is an efficient and safe method for the diagnosis of non-visible intrapulmonary nodules, especially for peripheral, sub-pleural nodules.”7
“The CT-guided placement of the pulmonary nodulemarker system used here offers a safe and accurate guide for the localization of small pulmonary nodules during thoracoscopic resection.“8

Order information
Lung Marker System
18 G puncture cannula and stylet with marking wire
Product code 272012 / 18 Gauge / 1.20 mm diameter / 120 mm cannula length
Product code 272015 / 18 Gauge / 1.20 mm diameter / 150 mm cannula length
Instructions for use
Lung Marker System